Parece que você está nos Estados Unidos
Temos um site diferente (www.q-bital.com) que melhor se adapta à sua localização
Dados recentes ilustram a dimensão do desafio. Só em março de 2026, houve mais de 2,4 milhões de atendimentos em emergências na Inglaterra, além de mais de 550 mil internações de emergência. Ao mesmo tempo, mais de 120 mil pacientes enfrentaram atrasos de mais de quatro horas desde o momento em que foi tomada a decisão de interná-los, incluindo dezenas de milhares que esperaram mais de 12 horas.
Na Escócia, o cenário é igualmente preocupante. Em fevereiro de 2026, houve mais de 122.000 atendimentos em emergências, com apenas 66,41% dos pacientes atendidos, tratados ou liberados em até quatro horas.
Esses não são números isolados. São indicadores de um desafio sistêmico que se estende muito além do próprio pronto-socorro.
O desempenho no atendimento de urgência e emergência é frequentemente enquadrado como um problema específico do pronto-socorro. Na realidade, trata-se de um problema de fluxo de pacientes em todo o percurso do paciente.
A pressão começa antes mesmo da chegada dos pacientes, com os tempos de resposta das ambulâncias e os atrasos na transferência de pacientes refletindo a disponibilidade de leitos nos hospitais. Ela continua durante a triagem, a avaliação e o tratamento, e muitas vezes é sentida com mais intensidade no momento da admissão, quando a disponibilidade de leitos se torna a principal limitação.
A alta hospitalar tardia é um fator contribuinte significativo. Na Escócia, quase 2.000 leitos hospitalares foram ocupados diariamente em fevereiro de 2026 por pacientes que estavam clinicamente aptos a receber alta, mas não conseguiam fazê-lo, com um atraso médio de 29 dias.
Quando o fluxo diminui em qualquer ponto, o impacto é sentido em todos os lugares. Ambulâncias formam filas, os serviços de emergência ficam lotados e os pacientes esperam mais tempo para receber atendimento.
Um dos sintomas mais visíveis e preocupantes dessa pressão é o aumento do chamado atendimento em corredores.
Uma resposta recente do governo levou ao envio de especialistas do NHS (Serviço Nacional de Saúde do Reino Unido) para lidar diretamente com essa questão, reconhecendo tanto sua prevalência quanto seus riscos. O Órgão de Investigação de Segurança dos Serviços de Saúde foi claro em suas conclusões: ambientes de atendimento temporário, incluindo corredores e espaços não clínicos, apresentam preocupações significativas em relação à segurança do paciente. Essas preocupações incluem dificuldades no monitoramento de pacientes, acesso limitado a equipamentos como oxigênio, aumento do risco de infecção e redução da privacidade e dignidade.
O atendimento em corredores não é uma solução. É um sintoma de capacidade insuficiente e fluxo restrito.
Para solucionar esse problema, são necessários mais do que ajustes operacionais. É preciso criar ambientes adequados e clinicamente compatíveis que possam absorver a demanda com segurança.
A política nacional está cada vez mais alinhada com essa realidade.
O Plano de Atendimento de Urgência e Emergência do NHS para 2025/26 estabelece uma ambição clara de reduzir as longas esperas, melhorar os tempos de transferência de pacientes das ambulâncias e eliminar o atendimento em corredores. Fundamentalmente, ele é apoiado por um investimento de capital significativo, incluindo mais de £ 370 milhões para expandir a capacidade por meio de novas unidades de Atendimento de Emergência no Mesmo Dia, centros de tratamento de urgência e outras infraestruturas.
Essa é uma mudança notável. Ela reflete um reconhecimento crescente de que o desempenho operacional não pode melhorar sem capacidade física para suportá-lo.
O destacamento de especialistas do NHS para lidar com o atendimento em corredores reforça ainda mais essa direção. O foco não está apenas na melhoria dos processos, mas em garantir que os pacientes sejam tratados em ambientes seguros e adequados.
A questão crucial para os líderes da área da saúde não é se é necessária capacidade adicional, mas onde ela terá o maior impacto.
A experiência em todo o NHS demonstra que intervenções direcionadas em pontos críticos podem transformar o fluxo de pacientes:
As instalações de transferência de ambulâncias podem reduzir os atrasos na entrada, permitindo uma resposta mais rápida das equipes e melhorando a capacidade de resposta do sistema.
Ambientes de triagem e encaminhamento, como Unidades de Atendimento a Lesões Leves e instalações de Atendimento de Emergência no Mesmo Dia, podem garantir que os pacientes sejam direcionados para o caminho mais apropriado desde o início.
Espaços adicionais nas enfermarias e salas de espera para pacientes que recebem alta podem aliviar a pressão na entrada dos fundos, liberando leitos e permitindo a admissão oportuna de pacientes provenientes dos departamentos de emergência.
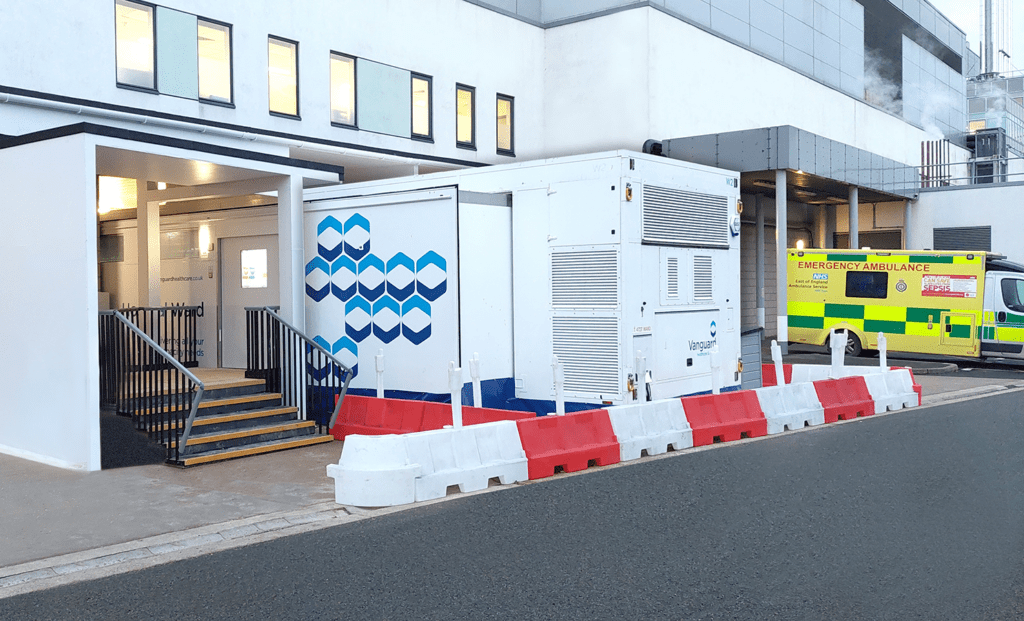
Essas não são soluções teóricas. No Hospital Municipal de Peterborough, uma unidade de transferência de pacientes das ambulâncias auxiliou no tratamento de mais de 15.000 pacientes, reduzindo atrasos e melhorando o fluxo de atendimento. No Royal Infirmary de Edimburgo, uma Unidade de Atendimento a Lesões Leves, localizada no mesmo prédio, agora atende até 100 pacientes por dia, aliviando a pressão sobre o Pronto-Socorro e melhorando a priorização dos pacientes.
O que esses exemplos demonstram é que a capacidade, quando implantada no local certo, tem um impacto desproporcional no desempenho.
O tempo é um fator crítico. Projetos de investimento tradicionais podem levar anos para serem concluídos, enquanto as pressões operacionais são imediatas.
É aqui que a infraestrutura flexível desempenha um papel vital.
As instalações de saúde móveis e modulares podem ser implantadas rapidamente, muitas vezes em questão de semanas, proporcionando ambientes clínicos totalmente compatíveis com as normas e que se integram às instalações hospitalares existentes. Elas permitem que os Conselhos e Fundações de Saúde respondam a picos sazonais, apoiem programas de transformação a longo prazo e mantenham fluxos de pacientes seguros durante períodos de alta demanda.
É importante destacar que também estão alinhadas com os modelos de financiamento atuais, oferecendo flexibilidade tanto no orçamento de receitas quanto no de capital.
Os desafios enfrentados pelos serviços de urgência e emergência são significativos, mas não são insuperáveis.
Agora existe um alinhamento claro entre as políticas, o financiamento e as prioridades operacionais. O foco está se voltando para a criação da capacidade necessária para oferecer atendimento seguro e oportuno em todo o percurso do paciente.
Para os líderes da área da saúde, a oportunidade reside em traduzir essa direção em ações práticas. Isso significa identificar onde as limitações de capacidade são mais críticas e implementar soluções que possam fazer uma diferença imediata e duradoura.
Se você está revisando sua capacidade de atendimento de urgência e emergência ou planejando como lidar com as pressões atuais, convidamos você a explorar como uma infraestrutura flexível pode apoiar sua organização.
Você pode baixar nossa brochura sobre Atendimento de Urgência e Emergência aqui:


Vanguard Soluções de Saúde
Unit 1144 Regent Court, The Square, Gloucester Business Park, Gloucester, GL3 4AD
Temos um site diferente (www.q-bital.com) que melhor se adapta à sua localização